Driving new AFib treatments by identifying its source
A heart physician and a scientist are gaining momentum in the quest to understand and treat atrial fibrillation, a common heart condition with devastating effects on millions across the globe.
Vadim Fedorov, PhD, was only 6 years old when his grandfather was hospitalized with a heart attack in their hometown of Voronezh, Russia, but even now, he can recall the incident in vivid detail.
“Sitting at my grandfather’s bedside in the hospital, I promised him that someday, I would find a way to make his heart beat forever,” Fedorov says.
Dr. Fedorov’s grandfather eventually recovered, but he lost his father and grandmother to sudden cardiac arrest in the years that followed. He enrolled in a Physics of Living Systems program at the Moscow Institute of Physics and Technology, resolved to develop technology that could help prevent cardiac death for families like his. And that’s exactly what he did.
Since he joined the Ohio State University College of Medicine Department of Physiology and Cell Biology in 2011, Federov has conducted pioneering research in cardiac arrhythmia, a condition that occurs when the electrical impulses that coordinate heart rhythms misfire, causing the heart to beat too quickly or too slowly. If not treated, cardiac arrhythmia can be fatal.
Dr. Federov is also the Corrine Frick Research Chair in Heart Failure and Arrythmia. Not long after he joined the faculty, he met a kindred spirit in John Hummel, MD, an electrophysiologist at The Ohio State University Wexner Medical Center and Corrine Frick Chair in Cardiac Electrophysiology at the College of Medicine. A specialist in the treatment of cardiac arrhythmia, particularly an arrhythmia called atrial fibrillation (commonly known as AFib), Dr. Hummel is always looking for new strategies to improve patients’ outcomes and quality of life.
His initial meeting with Dr. Fedorov would prove to be fortuitous. For over a decade now, the two have worked together to uncover the hidden sources of atrial fibrillation and pave the way to more effective treatment for millions.

Ending the debate
AFib is a rapid, irregular heartbeat that originates from the two upper chambers of the heart called the atria. Instead of coordinating with the ventricles — the two lower chambers — to maintain a steady heartbeat, the atria go rogue. Untreated, AFib can lead to blood clots, stroke and heart failure.
Ablation uses heat to interrupt the abnormal electrical activity that sustains atrial fibrillation. It’s a common procedure and is considered the standard of care in the treatment of AFib. Dr. Hummel and his colleagues observed that while they could successfully treat some patients by using the well-defined technique of eliminating triggers from the pulmonary veins, this approach was inadequate for others.
“For more than a decade, there was substantial controversy over whether or not there were sites outside the pulmonary veins that sustained AFib,” Dr. Hummel says. “The topic was of little interest to the world at large, but it was a burning issue within my field. Based upon existing studies in animals by other investigators, we suspected that if these sites did exist, we could target them and make them electrically silent, effectively eliminating AFib in many patients.”
The debate over whether these sites exist in humans ended in a laboratory on Ohio State’s campus, where Dr. Fedorov and his team developed a novel human heart model that provides a rare glimpse into the inner workings of the heart.
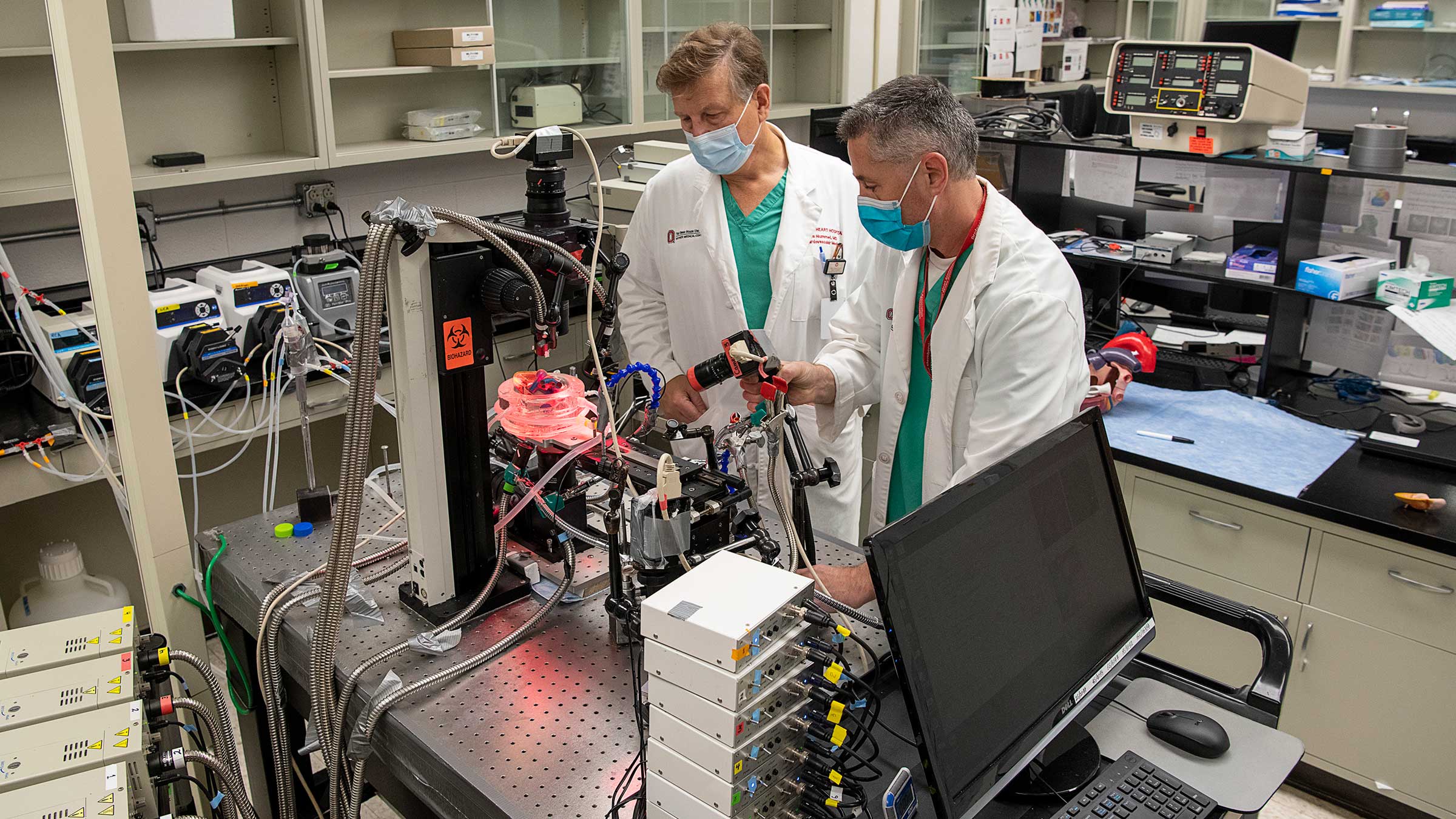
Visitors who don’t know that the heart can beat outside of the human body are in for a shock when they visit the Fedorov Laboratory. On any given day, they may find a glass chamber containing a recently donated human heart perfused with (bathed in) a warm oxygenated solution.
This solution stimulates blood flow, allowing the heart to beat for at least 12 hours with the same rhythm as when it was inside the donor’s body.
Many of these hearts come to the Fedorov Lab from patients undergoing a heart transplant at The Ohio State University Wexner Medical Center Richard M. Ross Heart Hospital, who’ve elected to donate their diseased heart to science, while some hearts are donated through Lifeline of Ohio.
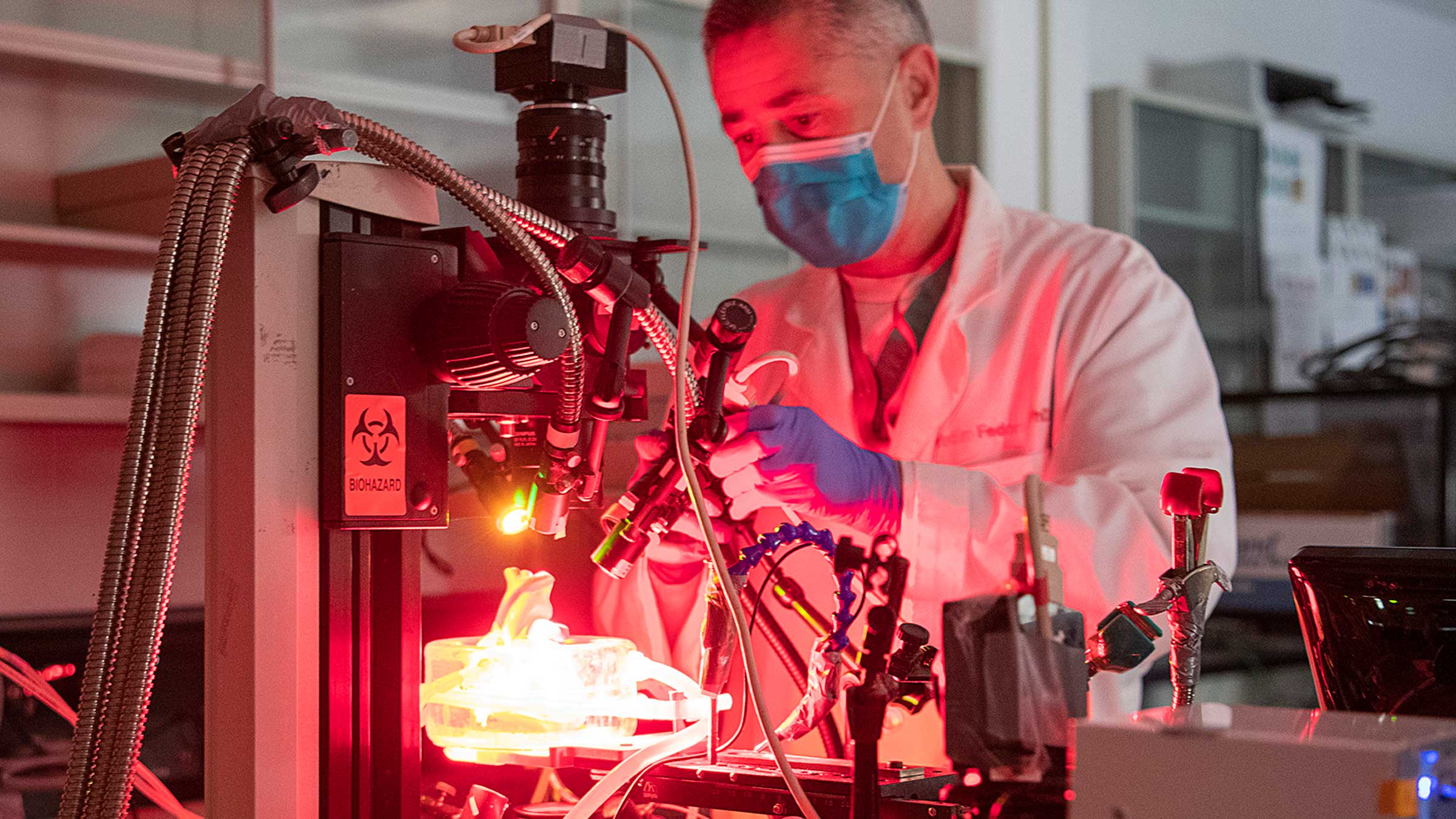
Once the donated heart is resuscitated, Dr. Fedorov and his team place atrial tissue in a perfusion bath surrounded by four ultrasensitive infrared cameras. They then inject fluorescent dye that can sense electrical activity straight through the atrial wall.
The combination of the dye and the infrared light reveals an unprecedented level of information about the structure and electrical function of the heart. While current clinical imaging displays 200 recordings across the heart, Dr. Fedorov’s imaging system displays 40,000.
“Essentially, this imaging allows us to see how electricity spreads across the structure of the human heart in 3D,” Fedorov says.
“It confirmed the presence of something we were already seeing in animal models: re-entrant drivers in the atria. These are small sites outside the pulmonary veins where we can observe the abnormally fast electrical activity that sustains AFib.”
Published in the European Heart Journal in 2015, Dr. Fedorov’s findings definitively established the existence of re-entrant drivers in the atria, and this ushered in a new era for translational patient care.
Dr. Hummel remembers meeting Dr. Fedorov in 2013 at a professional lecture Dr. Fedorov delivered on disease of the sinus (sinoatrial) node, the natural pacemaker of the heart. Dr. Hummel immediately recognized the translational potential of the imaging technology Fedorov was describing, calling it a “feather in the cap of Dr. Fedorov and Ohio State.” From that day on, a fruitful collaboration emerged.
With the exception of one overseas medical facility, Ohio State is the only health center in the world employing this technology in human hearts. By inducing AFib in a donated heart, Dr. Fedorov can gather information that illuminates a better treatment strategy for patients.
To date, Fedorov and Dr. Hummel have co-authored close to 30 research articles, several of which focus on what AFib re-entrant driver sites look like anatomically with high-resolution, 3D magnetic resonance (MRI) imaging. They reported finding that re-entrant drivers aren’t always a closed loop, as previously thought, but are instead more like hubs of electrical activity that resemble tornadoes.
Importantly, the translational findings from Drs. Fedorov and Hummel’s team on human atrial fibrillation mechanisms were recently recognized and highlighted by an international panel of leading clinical and basic AFib experts at the Position Paper from the International Working Group of the Signal Summit, where both investigators served as expert panelists and co-authors.
“Everyone likes to talk about translational research, but it’s rare to find such a straight line of connection between two labs,” Dr. Hummel says. “It’s been an exciting partnership that relies on the strength of a much larger team than the two of us.”

New frontiers in AFib
Together with the colleagues in their respective labs, and in collaboration with the Bob and Corrine Frick Center for Heart Failure and Arrythmia, Drs. Fedorov and Hummel are changing how atrial fibrillation is studied. Despite their accomplishments, they’re quick to point out that they have just as many questions as answers.

“We’re still in the process of learning what makes some regions of the heart more susceptible to becoming a hub for AFib,” Dr. Hummel says.
“We need to find out what makes some driver sites more and less important, not just electrically but anatomically. If two patients have a different number and location of driver sites, can we determine that further ablation is wasted effort in one case but not the other?”
In May, Dr. Fedorov led a study on how genes tend to cause women to have faster heartbeats and men to develop AFib.
The research shows that the heart’s sinoatrial (sinus) node, runs on different gene blueprints in men and women. It was published in the American Heart Association’s Circulation: Arrythmia and Electrophysiology journal.
Dr. Fedorov hopes the findings will help find more personalized, patient-specific approaches to treating heart rhythm disorders.
Building on this discovery, Dr. Fedorov, together with Dr. Hummel and clinical collaborators through the direct support of the Dorothy M. Davis Heart and Lung Research Institute, is continuing investigations into sex- and age-specific predictors of atrial fibrillation and the development of patient-specific therapeutic strategies. These ongoing studies aim to uncover how biological sex and aging influence cardiac structural and electrical remodeling — key steps toward more precise, personalized interventions for heart rhythm disorders.
Ultimately, Drs. Hummel and Fedorov aim to develop therapeutic drugs, ablative therapies and prevention strategies to target AFib in individual patients. “The more we can understand AFib in the context of specific health conditions, the more we can tailor our treatments to individual patients,” Dr. Fedorov says. “This is the next frontier in patient care.”
Ingredients for success
It’s common for Dr. Fedorov to spend the night in his lab. When a donated heart arrives, he and his team frequently work 24-hour shifts to gather and analyze data.
Their work is relentless and rewarding in equal parts. “What we do requires sacrifice, but it’s worth doing to benefit cardiac patients,” Dr. Fedorov says. “Dozens of people are involved in every research project we undertake, and their hard work has gained international recognition.”
The Ohio State Wexner Medical Center has all the right pieces for success in the battle against AFib: a large group of electrophysiologists, a world-class physiologist who specializes in cardiac arrhythmia, a one-of-a-kind heart model and experts in cardiac genetics and imaging.
“We’re well-positioned to accelerate the process of translating basic science into clinical studies and outcomes,” Dr. Hummel says. “That’s what gets me out of bed in the morning. Our work may not put AFib in the rearview mirror just yet, but it will help a lot of people.”
With plenty of unanswered questions before him, Dr. Fedorov anticipates many more nights working in his office and lab.

“When I think about my grandfather in that hospital, or when I think about the loved ones so many families like mine have lost, that keeps me going through the long days and nights. We have to press on.”

Take charge of your heart health
Learn more about the causes of atrial fibrillation (AFib) and treatment options available at Ohio State.
Take charge today